By Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS,
C-IASTM, NASM-CPT
The shoulder is a complex joint possessing a large degree of freedom that can easily break down. Familiarizing yourself with the interarticular and extraarticular supporting parts will enable you to understand the ‘why’ behind these parts. As well as why shoulder impingement syndrome and rotator cuff tears are more common than you think. This article will review the foundational anatomy and biomechanics of the shoulder, discuss what shoulder impingement is and teach the ‘why’ behind program design.
Learning Objectives:
1. Identify the cause of rotator cuff dysfunctions and contributing factors.
2. Identify, which exercises, are safe vs. unsafe based on biomechanics and science when working with impingement clients.
3. Identify the importance behind scapular stabilization exercises with gaining hands-on experience during the session.
4. Understand the ‘why’ behind design programs that include scapular stabilization core and functional strengthening using a multitude of exercise equipment.
Functional anatomy
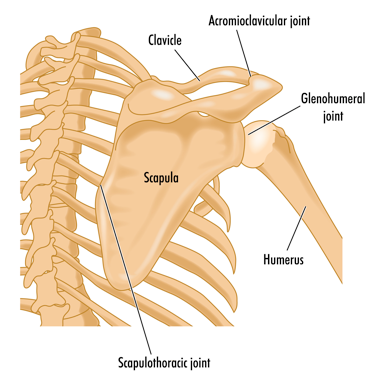
There are four primary joints within the shoulder. They include the sternoclavicular joint (SC), which is composed of two relatively incongruent surfaces, the medial end of the clavicle and posterior lateral aspect of the manubrium and first rib. The acromioclavicular joint (AC) which is by the lateral end of the clavicle acromion. The scapulothoracic joint: is formed where the scapula articulates (meets) the thorax (upper back). Finally, the glenohumeral joint: is formed by an anterior and posterior joint capsule, ligaments that provide static stability and surrounding muscles, which can be seen in figure one.
Biomechanics of shoulder
During side raising of the shoulder, the humerus slides down in the glenoid cavity(vertical arrow), while the scapula upwardly rotates on the thorax

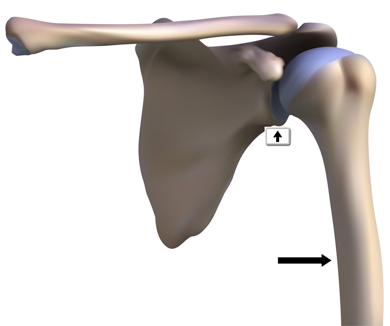
The upwardly rotation of the scapular on the thorax is called the scapulohumeral rhythm (SHR) as seen in figure four. Biomechanically, there is 120 degrees of movement that occurs at the glenohumeral joint and 60 degrees at the scapulothoracic joint (2:1 ratio)

Shoulder impingement
Pathophysiology/mechanism of injury: Shoulder impingement (SI) is the mechanism in
which the supraspinatus tendon of the rotator cuff becomes impinged as it passes through a
narrow bony space called the sub acromial space. With repetitive movement, the supraspinatus
tendon can become irritated and inflamed. SI can also be caused by a decrease in posterior
capsule mobility and weakness of scapulothoracic musculature.
Evidenced based research has shown that shoulder impingement is a common condition
believed to contribute to the development or progression of rotator cuff disease(Ludewig, P. 2011).
- Decrease in sub acromial space comprises the supraspinatus tendon, predisposing it
to micro tears leading to degeneration and ultimately tearing. - Tightness of the posterior capsule causes the humerus to migrate anterosuperior into
the AC joint. - Weakness of scapulothoracic muscles leads to abnormal positioning of the scapula.
Common signs and symptoms: Clients will complain typically of pain in the front of the shoulder, described as deep, dull ache with stiffness. Reaching overhead and behind one’s back will elicit pain.

Contributing risk factors: Poor posture, repetitive overhead work, and tight posterior capsule are some contributing factors. Per the research, the development of SI has been correlated to abnormal muscle activation. Specifically, those with SI, present with the overactive upper trapezius and underactive lower trapezius muscles (Chester, R., et al. 2010).
Physical therapy management: The goal with physical therapy is to restore scapular mobility, followed with stretching to restore full range of motion. Strengthening focuses on targeting the weaker upper posterior musculature that includes rhomboids, low trapezius, external rotators, and serratus anterior muscles. Then the patient is taught scapular stabilization and dynamic strengthening exercises.
Program design and exercise prescription for the impingement client
Once discharged from physical therapy, transitioning to the gym should be simple, and based on science, not guessing. The focus on post rehabilitation training is to strengthen the scapular stabilizers (rhomboids, low trapezius, posterior deltoid, and external rotators) and posterior shoulder. Core strengthening should progress from static to dynamic exercises.


Upper body exercises that are safe based on biomechanics include:
- Low trapezius pull downs (figure 7) with cable standing or tubing, depresses and retracts the scapula, unloading the anterior shoulder, improving posture and posterior stability.
- Seated mid row (figure 8), one arm dumbbell row, seated reverse flyes
(posterior deltoid) strengthens the weaker phasic muscles of the posterior chain. - External rotation with cable, seated reverse flies, seated dumbbell side raises.
- Core strengthening exercises that are safe include but not limited to; standing trunk rotation with cable/tubing, diagonal with cable tandem in place lunge, planks, planks with ball, trunk rotation with forward lunge.
Exercises that are contraindicated include with rationale:
- Seated dumbbell shoulder press (creates excessive load to the medial deltoid).
- Lat pull downs behind the head (at end or range places greatest stress on all
glenohumeral ligaments as well as on the labrum).
- Upright row (at end of range-shoulder is maximally internally rotated which places
stress on all glenohumeral ligaments, labrum, and connective tissue).
Shoulder impingement is a common shoulder conditions that a fitness professional may encounter. Understanding the anatomy, biomechanics, and proper program design with evidenced based training strategies will provide you with a better understanding to work with clients.
Contact National Personal Training Institute to learn more about our personal training programs and more!
References
Bernhardsson, B., et al (2012), ‘Evaluation of an exercise concept focusing on eccentric strength training of the rotator cuff for patients with sub acromial impingement syndrome, Clinical Rehabilitation, pp. 1-9.
Chester, R., et al. 2010, ‘The impact of subacromial impingement syndrome on muscle activity patterns of the shoulder complex: a systematic review of electromyographic studies’
BMC Musculoskeletal Disorders, vol. 11, issue 45, pp. 1-12.
Holmgren, T., 2012, ‘Effect of specific exercise strategy on need for surgery in patients with sub acromial impingement syndrome: randomized controlled study,’ British Journal of Medicine,
pg. 344.
Kuhn, J., 2009, ‘Exercise in the treatment of rotator cuff impingement: A systematic review and a synthesized evidence-based rehabilitation protocol,’ Journal of Shoulder Elbow Surgery, vol. 18, pp. 38-160.
Ludewig, P., 2011, ‘Shoulder Impingement: Biomechanical Considerations in Rehabilitation,’
Journal of Manual Therapy, vol. 16, issue, pp. 33–39.
Chris Gellert, PT, MMusc & Sportsphysio, MPT, CSCS, C-IASTM, NASM-CPT
Chris is the CEO of Pinnacle Training & Consulting Systems (PTCS). Chris is both a dynamic physical therapist with 19 years experience, and a personal trainer with 20 years experience, with advanced training, has created 16 home study courses, is an experienced international fitness presenter, writes for various websites and international publications, consults and teaches seminars on human movement. For more information, please visit https://www.nationalptiglobal.org/therapeutic–health-care/certified-post-rehabilitation-specialist-cprs-certification/7314.

